So this is menopause. You are 52 years old and have not had a period in a year. That’s good. You are still having some hot flashes, but generally, they are not too bad. You wake up early too often, and that makes you tired during the day. What worries you is this – your mother is 77. She just fell and broke her hip. Her doctor says she has osteoporosis. What can you do to keep that from happening to you in the future?
Doctors sometimes prescribe the hormones estrogen and progestin, in a treatment called hormone replacement therapy (HRT), to ease the signs of menopause. It may also protect you against more serious illnesses in the future. Many women take HRT. Some women should not. It may or may not be the right choice for you. This area has been one of extreme controversy since 2002 when a large medical study determined that HRT could increase Breast Cancer in menopausal women. The risk of stroke and heart attack was also increased. However, in 2006, another large study showed that women who have had a hysterectomy do well with just estrogen replacement and receive all of the benefits without risks other than the same risks they would suffer if taking birth control pills. In any case, consulting a physician that you trust in this area (even if it means a second opinion or a trip to a University Medical Center) is a good idea. Treatment has to be individualized.
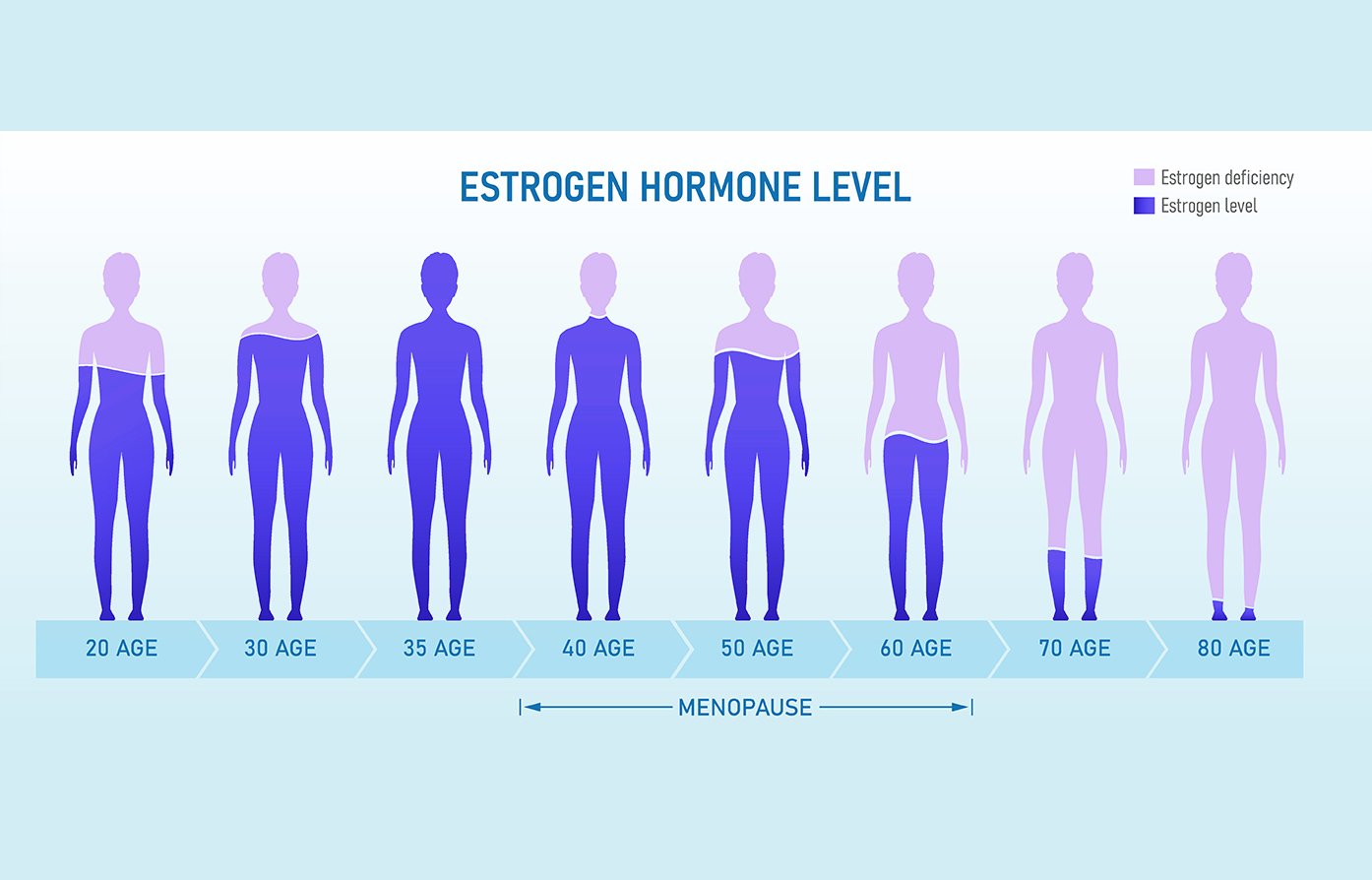
Now first, it’s a good idea to know what happens to your body with menopause. At this time, your body makes less of the female hormones, estrogen and progesterone. After menopause, you are free from concerns about monthly menstrual periods and getting pregnant. But during the years around menopause, you might have annoying symptoms. These may include hot flashes (a sudden flush or warmth, often followed by sweating), sleep problems, lack of sex drive and vaginal dryness. Many women have little or no trouble with menopause. Some have moderate to severe discomfort.
Estrogen loss also puts you at risk for more serious health problems. These include heart disease, stroke (which may be offset by the increase of stroke-taking estrogens), and osteoporosis. Heart disease is the leading cause of death for women over the age of 50. It kills more women than lung and breast cancer combined.
Bone loss is common as people age. However, if there is a great loss, osteoporosis may develop. This is a serious condition. Bones weaken and break easily. It threatens about 28 million Americans. Eighty per cent of them are women, and most are over 50 years of age. Estrogen replacement therapy has been proven to protect women from osteoporosis.
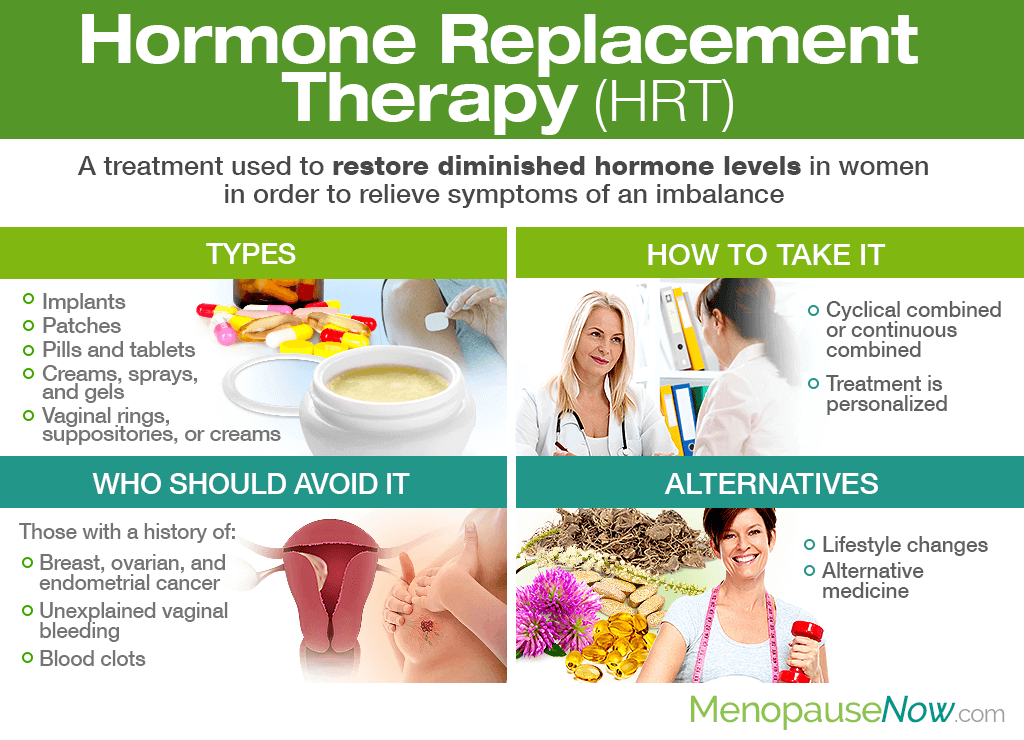
What Is HRT?
Doctors usually prescribe HRT which combines estrogen and progestin (a form of progesterone). Estrogen can and should be used alone (estrogen replacement therapy or ERT) for women who have had their uterus, including the cervix, removed (by a hysterectomy).
Estrogen alone comes in many forms. You can use the pill or tablet form, vaginal creams, vaginal ring inserts, implants, or shots. There are also patches that stick to the skin. The body absorbs estrogen from the patch through the skin. Progestin usually is taken in pill form, sometimes in the same pill as the estrogen. It is also available as an IUD (intrauterine device), a vaginal gel, and shots.
The form your doctor suggests may depend on your symptoms. For instance, estrogen creams are used for vaginal dryness. The vaginal ring insert treats vaginal dryness and may help urinary tract symptoms, such as problems holding urine. Pills or patches, however, are used to provide additional relief from menopause symptoms such as hot flashes or to prevent bone loss.
There are different schedules for taking HRT in pill form. You could take estrogen every day for a set number of days, add progestin for 10-14 days, and then stop taking one or both for a specific period of time. You would repeat the same pattern every month. This cyclic schedule often causes regular monthly bleeding like a light menstrual period. Or you could take estrogen and progestin together every day of the month without any break. This continuous pattern can stop monthly bleeding after about six months of treatment. However, problem spotting may continue for longer. Talk with your doctor about the schedule that is best for you.
Recurrent Vasomotor Symptoms Following the Discontinuation of Postmenopausal Hormone Therapy Two recent articles in the Journal of the American Medical Association bring much-needed attention to an increasingly common clinical scenario: the recurrence of menopausal symptoms after discontinuation of postmenopausal hormone therapy (HT). These articles underscore the need for clinicians to regularly follow up with patients experiencing menopausal symptoms and to carefully evaluate each patient's unique needs in the context of evolving data on the risks and benefits of HT. In the April 13, 2005 issue of Clinical Crossroads, an article provided a follow-up on the case of a now 62-year-old woman who suffered severe hot flushes following her attempt two years ago to discontinue unopposed estrogen therapy.1
She had used estrogen therapy for symptom relief since undergoing a hysterectomy and bilateral salpingo-oophorectomy at the age of 40 years. Her decision to discontinue HT after 20 years of use was based on her "increasing level of concern about her family history of breast cancer and the risks of HT that she had been reading about in the lay press."2 Although this patient reported that it was very difficult to tolerate the symptoms that she encountered in her attempt to discontinue HT, she was advised to again try to taper her estrogen although over a more extended period of time. The rationale for this advice was "growing concerns about the potential increased risk of breast cancer risk and coronary events in users of hormone therapy based on the Heart and Estrogen/Progestin Replacement Study, other published randomized trials, and early reports from the Women's Health Initiative."2 In this follow-up two years later,1 we learn that, over a one-year period, the patient tapered first to a daily low dose and then gradually tapered to every other and then every third day before stopping HT. However, she still reports hot flushes that are difficult to tolerate. At the same time, she is frightened to resume HT: "I am off the hormone therapy completely now...I know my life would be so much easier if I still took it. I felt so good when I was on it. I shouldn't have taken it, but I did what I thought was right at the time...I don't know how much damage I've caused to my body. I have to deal with that now. The hot flashes are quite frequent. I have hot flashes every hour. They last 2 to 3 minutes...I don't wish this on my worst enemy. It takes a great deal of willpower to stay off the estrogen, but I keep telling myself I should. I tried soy, but that did nothing. Someone mentioned herbal things, but I just don't feel like trying new things when I am taking other medication...I don't know what the next step is. There really isn't guidance out there; people out there are just guessing. If the doctors and the researchers can realize that it's true suffering, it's not just "she'll get over it"-it's not like that. It really makes an impact on your personal life. I'm standing here right now just dripping. It just pulls you down, especially as you get older. Women don't need this on top of everything else. I would like to feel the best I possibly can. I want to get the most out of life and enjoy my family."
Clearly, this patient's words reveal how uncomfortable and guilty she feels, and how desperate she is to obtain relief. Data published in 2004 from the WHI on the risks and benefits of unopposed estrogen therapy3 are especially relevant for this patient and the results should be shared with her at this 2-year follow-up. These results from the WHI estrogen-alone clinical trial are based on outcomes from nearly 12,000 women with prior hysterectomies who were randomized to receive either conjugated equine estrogens (CEE) or a placebo. After a median of 6.8 years of unopposed estrogen therapy, there was no increased risk of cardiovascular events and a trend towards a reduction in the risk of breast cancer that just failed to reach statistical significance. An increased risk of stroke was, however, associated with the use of unopposed estrogen. Carefully reviewing the results of the WHI estrogen-alone trial with this patient and relating the findings to her needs enables the physician to reassure her, offer immediate relief of symptoms, and assuage her guilt. This distraught woman could find solace and comfort and safely return to HT by clarification of her risks and benefits in view of the most current and relevant scientific evidence. Of course, this patient may consider the evidence and decide not to restart HT, but her decision must be based on an accurate and comprehensive understanding of the risks and benefits of treating her menopausal symptoms with unopposed estrogen.
Patients such as this one who experience recurrent symptoms following discontinuation of HT are common, yet research is lacking on the prevalence, severity, and duration of these recurrent symptoms. Recently, women who had participated in the WHI estrogen plus progestin (E+P) clinical trial was surveyed about the symptoms they experienced after discontinuing their study medication (HT or placebo) when the study was stopped prematurely. The results of this survey, which was sent only to those women who were still taking study medication at the trial stop date, were published in the July 13, 2005 issue of JAMA.4 The survey found that 21% of the women who had been using E+P therapy during the trial reported moderate or severe vasomotor symptoms after discontinuing treatment. However, the rate of recurrent symptoms was substantially higher in the subset of women who were experiencing menopausal symptoms at the outset of the clinical trial-more than half of these women (55.5%) reported moderate or severe vasomotor symptoms after discontinuing HT. Interestingly, 5% of the women who had been on placebo during the trial reported moderate or severe vasomotor symptoms in the year following the trial stop date. As seen in the E+P group, being symptomatic prior to entering the clinical trial increased the likelihood of recurrent symptoms among the women in the placebo group. Unclear from these findings is whether the women in the placebo group who reported symptoms after the trial ended had also experienced symptoms during the trial or whether these women were more likely to be among the 11% of women who "crossed over" during the trial and initiated HT with their own physician. Thus, although these findings were dubbed the "placebo withdrawal effect" in a related editorial,5 other plausible explanations should be considered as well.#
Certainly, the average age of the WHI participants (69.1 years at the time the E+P study was stopped) and the small proportion of the WHI study population reporting menopausal symptoms at baseline limits the applicability of the survey's findings to the population of younger, symptomatic postmenopausal women most likely to receive treatment with HT. Despite these limitations, the study addresses an important clinical issue and provides information of value to practitioners. In the small group of women aged 55-59 years (n=598), the rate of recurrent hot flashes or night sweats after discontinuing E+P was 36%. Although not reported, the rate of recurrent symptoms was likely higher among women aged 55-59 years who reported menopausal symptoms prior to the start of the trial. While further research is needed to more accurately estimate the prevalence of recurrent symptoms in younger, symptomatic postmenopausal women, current evidence suggests at least one-third to one-half of these women can be expected to experience recurrent symptoms when HT is discontinued. Further research is also needed on the average duration of recurrent symptoms, the effects of various discontinuation strategies (eg, using lower doses, decreasing the number of days per week that HT is taken, or a combination of these strategies), and the usefulness of lifestyle strategies to manage recurrent symptoms (eg, drink more fluids, wear layered clothing). In the WHI survey, women with recurrent symptoms reported trying a number of lifestyle strategies to manage their symptoms and most women felt these strategies were "helpful." Interpretation of this finding is difficult, however, as the questionnaire gave respondents only three responses ranging from "helpful" to "made things worse" to describe their perceptions of these strategies.
In conclusion, the WHI investigators and the editors at JAMA are to be commended for facilitating scientific and clinical discourse on the recurrence of menopausal symptoms after HT discontinuation. The recent publications in JAMA provide an opportunity to remind clinicians that current recommendations for the use of HT are not simply to use the lowest effective dose for the shortest duration possible, but rather to use the lowest effective dose for the shortest duration needed to reach therapeutic goals.6,7 For the woman who continues to have disruptive vasomotor symptoms, therapeutic goals are not being met and the potential re-initiation of HT should be re-evaluated within the context of the risks and benefits for this individual patient.
Pros of using: HRT and ERT may improve mood and psychological well-being.
Cons of using:
ERT, especially without the use of progestin, increases the risk of cancer of the uterus (endometrial cancer).
HRT can have unpleasant side effects, such as bloating or irritability.
HRT and ERT may increase the risk of breast cancer; long-term use may pose the greatest risk.
In women at risk of blood clots, HRT and ERT may be dangerous.
What are SERMs?
SERMs (selective estrogen receptor modulators) are a new type of medicine. Raloxifene (approved by the Food and Drug Administration to prevent osteoporosis) and tamoxifen (approved for breast cancer treatment and prevention) are examples of SERMs. They are designed to do some of the good things estrogen does such as protecting bone density. However, they may not have some of the negative side effects. For example, tamoxifen appears to protect against developing breast cancer. Raloxifene does not seem to increase the chance of endometrial cancer as estrogen alone or tamoxifen might. Women on tamoxifen should see their gynecologist regularly to be sure their uterus is normal. These two SERMS do, however, have a risk of blood clots similar to estrogen. Also, raloxifene and tamoxifen can make hot flashes worse. Scientists are continuing to work on developing better SERMs to use for menopause in the future.
Should I Use Hormone Therapy?
This question is best answered after talking with your doctor (general practitioner, internist, or gynecologist). He or she can tell you if you should consider HRT or ERT. You probably should not use these supplements if you have liver disease, high levels of triglycerides (a type of fat in the blood), or a history of blood clots in your veins. Women with a family history of breast cancer might also want to get the opinion of their cancer doctor.
The first step is to decide how much you are bothered by menopause symptoms such as hot flashes. You will also need to think about your medical history, your risk of heart disease, osteoporosis, and breast cancer, and your family history of these illnesses.
Any decision about HRT or ERT that you make now is not final. You can start or end the treatment anytime, but if you stop it, the protective effects of these therapies will stop as well. Your decision about hormone therapy should be reviewed each year with your doctor at your annual checkup. After menopause, it is important to continue yearly breast and vaginal exams, Pap tests, and mammograms, as well as a general physical exam.